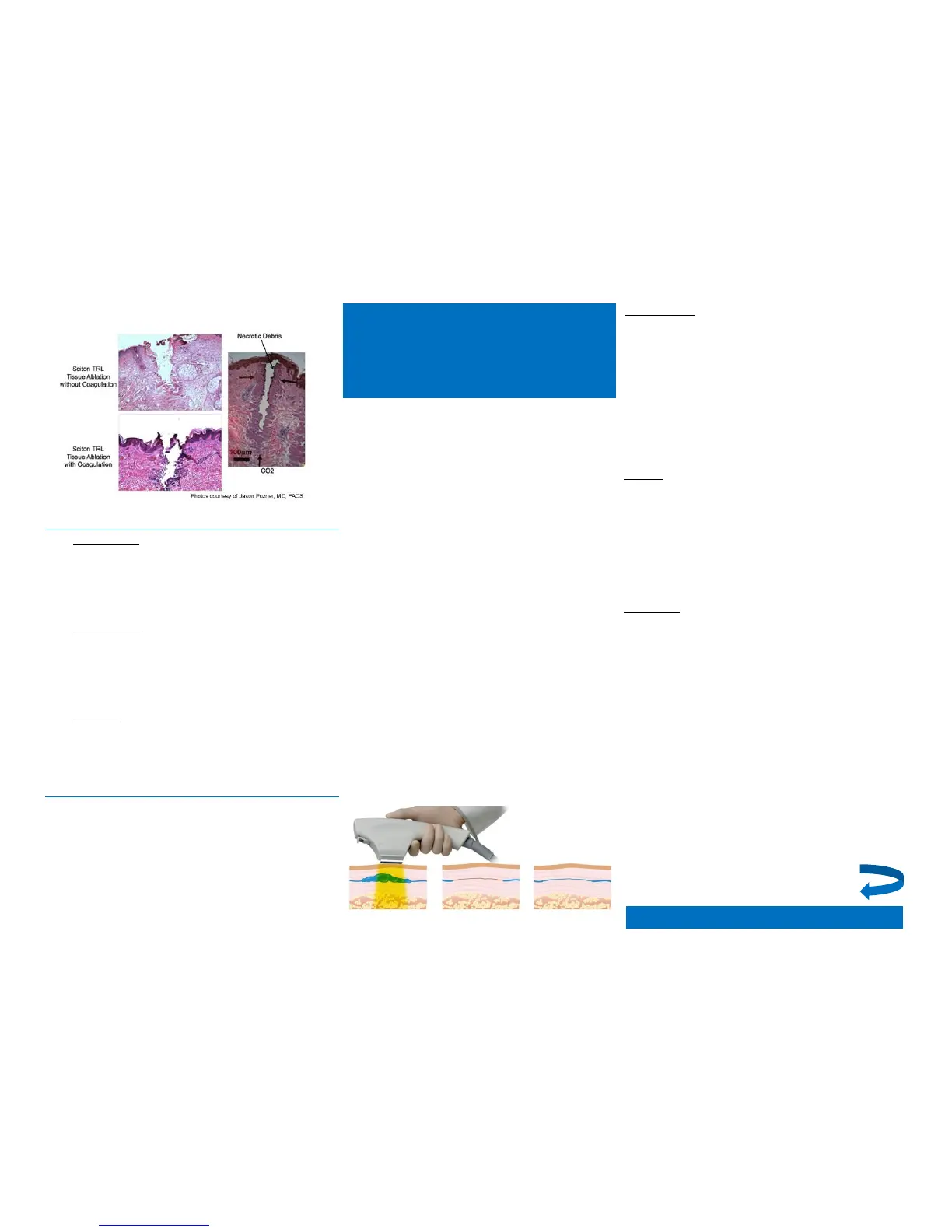
The graph shows a supra-ablative pulse (well above the ablation threshold) which
vaporizes tissue to a controlled depth, followed by a train of sub-ablative pulses, which
raise the tissue temperature
Post-Treatment
1. OBSERVATIONS
Pinpoint or punctuate bleeding during and
immediately following treatment. Erythema and
edema noted for approximately 12-48 hours after
treatment depending on depth and percentage of
area treated.
2. INTERVENTION
Cool compresses or ice packs can provide immediate
comfort after treatment. An occlusive barrier such as
Aquaphor will provide protection and comfort to
treated area and should be used until skin has
reepithelialised.
3. INTERVAL between ProFractional/ProFractional-XC
treatments is 2 - 6 weeks depending upon depth,
treatment area percentage and level of COAG, if
used.
Concurrent Procedures
2940 Er: YAG Contour TR ProFractional/ ProFractional-XC
treatments may be given in combination with other
procedures. If a patient is undergoing a BBL or MLP
procedure, these treatments should be performed before
the ProFractional/ProFractional-XC.
Check with manufacturer for guidelines on using injectables
in conjunction with 2940 Er:YAG Contour TRL
Safe Start Protocol for BBL
- Non-Ablative Vascular/Skin
Treatment
Filter selection
Refer to Vascular/Skin Treatment Starting Parameters
for appropriate filter selection.
For vascular lesions, flushing, blushing and/or rosacea
that resides deeper in tissue and for areas where these
conditions are more densely populated, a deeper
penetrating filter should be chosen. Melanin in the skin
competes with the targeted vascular lesions for
absorption of the BBL light. Therefore, a deeper
penetrating filter should be chosen for patients with
darker skin types
Fluence
Refer to Vascular/Skin Treatment Starting Parameters for
appropriate fluence selection.
Targets that have more dense vascularity absorb more
energy/heat and will reach higher temperatures.
Therefore, redder, more concentrated areas of vascular
lesions require less fluence than lighter coloured, less
concentrated areas of vascular lesions to reach the
same therapeutic level.
Pulse Width
Refer to Vascular/Skin Treatment Starting Parameters for
appropriate pulse width selection.
Pulse width should be shorter than the cooling time of the
target to make sure that all of the energy is confined to
the target. Smaller objects cool faster than larger ones.
Therefore, the smaller the vascular lesion being treated
the less time on, or a shorter pulse width. Conversely,
when treating a larger vascular lesion, a longer pulse
width should be selected to provide for a longer period
of heat delivery.
Vascular lesions with less dense vascularity will cool down
quicker than more densely pigmented ones. Therefore,
“lighter’, less concentrated vascular lesions should be
treated with shorter pulse widths and “redder”, more
concentrated lesions should be treated with longer pulse
widths. Darker skin absorbs more light and heats to a
higher temperature, therefore pulse width should be
longer for darker skin.
The BBL Non-Ablative Vascular/Skin
Treatment Protocol is effective for treating
redness, flushing, blushing, rosacea, red scars
and broken capillaries.
The theory of Selective Photothermolysis
explains how wavelength, energy and pulse
width in relation to Thermal Relaxation Time
(TRT) all play a role in the destruction of a
target and the preservation of surrounding
tissue.
Using the theory of selective
photothermolysis, benign vascular lesions can
be treated with the appropriate BBL filter and
settings that will cause selective absorption of
light in the blood that is flowing through the
targeted vessel. The absorption converts light
into heat energy, which raises the
temperature of the blood.
Heat is conducted to the lining of the vessel
wall leading to its injury. This results in slow
elimination of the vascular lesion by the
macrophages of the immune system. All of
this should happen selectively and without
damage being done to the epidermis or
surrounding tissue.
Turn back for
more information

 Loading...
Loading...