– 41 –
NOTE:
One may choose to leave the OF-G11 adapter attached to the endoscope
during conventional air insufflation using the air/water feeding valve.
However, the luer sideport of the OF-G11 must be capped.
Similarly, for normal water delivery, the air pump must be turned ON and
the plastic luer lock cap must be secured to the OF-G11 adapter.
6) The laser probe should be introduced through the endoscope in the same manner
as described for biopsy forceps in section 3-4.
7) The position of the active portion of the laser probe should always be clearly
visualized before laser equipment is activated.
8) It should be recognized that a variety of factors can affect the quality of the video
endoscope image during laser use. Intensity of the aiming beam, high power
setting of the laser, close distance of laser ber to endoscope tip, excessive tissue
burning, can each adversely inuence image quality. To obtain optimum results, it
is recommended that the power settings of the aiming beam and laser be adjusted
to minimal levels capable of achieving the desired clinical effect.
9) Follow standard hospital protocol regarding safe-use of lasers, including the
wearing of safety eyewear.
CAUTION:
Prior to activation of the laser, make sure that the laser fiber exits the
distal channel opening of the endoscope. Failure to conrm activation and
deactivation of the laser could result in endoscope damage.
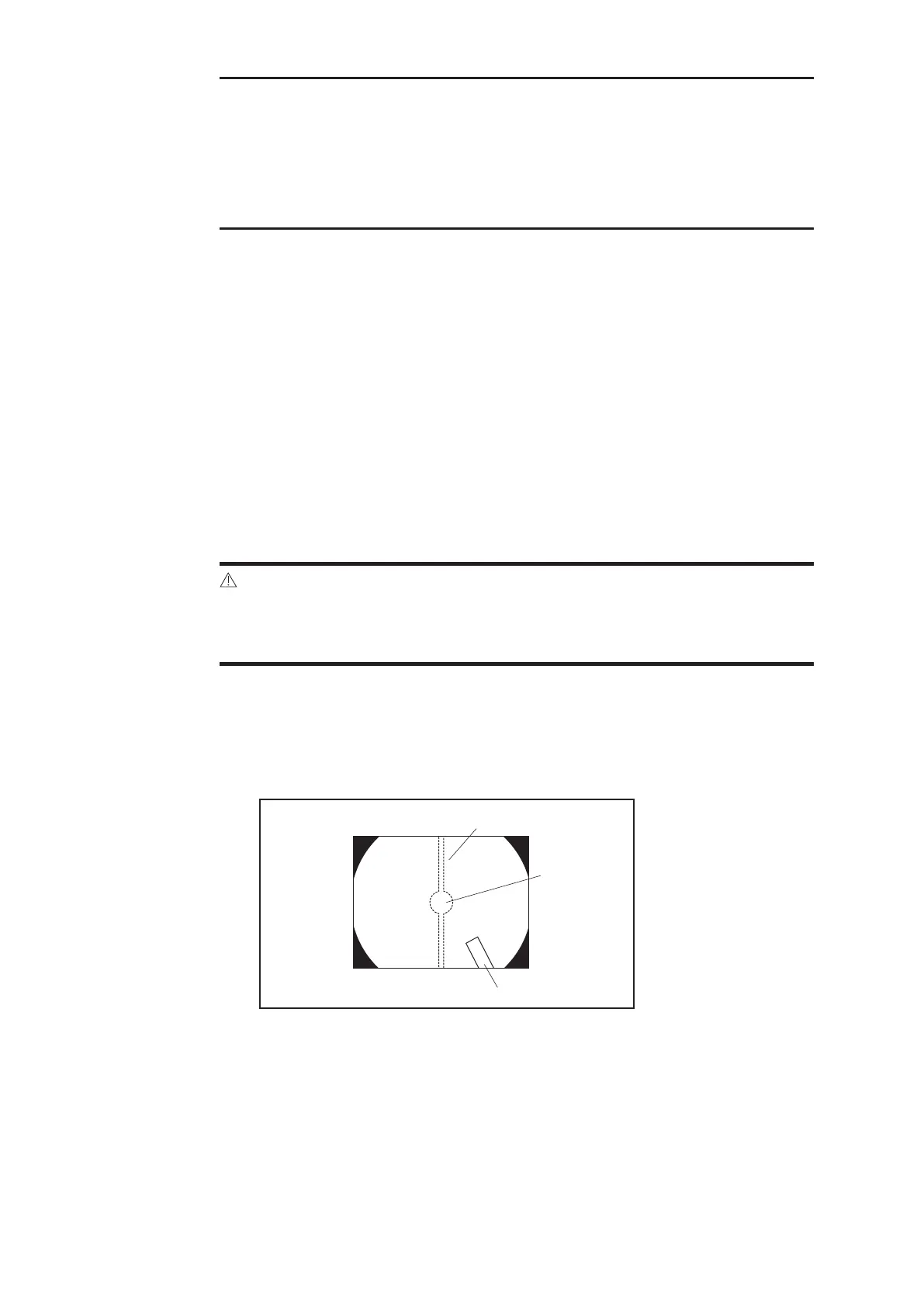
10) Should the distal tip of the endoscope be moved closer than 20mm from the
irradiated tissue surface, the aiming beam may create a “smear” in the image
as shown in gure 3.12. If this smear affect becomes too severe and distorts the
visual eld, the intensity of the aiming light should be decreased.
(1) Smear
(2) Irradiated Area
(3) Probe
Figure 3.8
 Loading...
Loading...