D1091 Rev.M August. 2016
TREATMENT TECHNIQUE – 1064 NM VASCULAR WITH COOLVIEW HANDPIECE
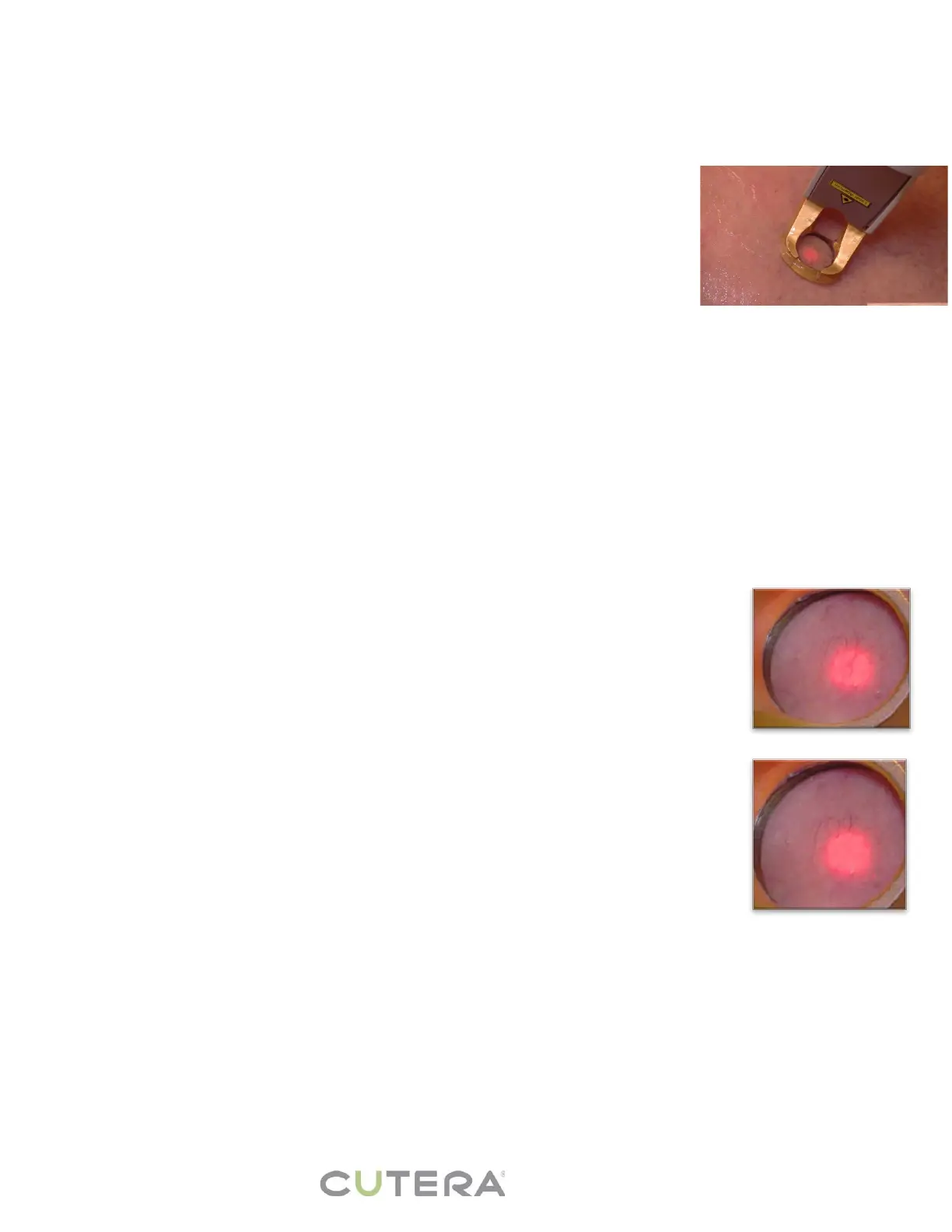
• WARNING: The red diode aiming beam in the sapphire window should be in full contact with the skin before, during,
and after the laser pulse.
o Pay close attention when treating over the nose or curved areas to ensure full contact with the window
where the red aiming beam is present.
o Consider using smaller spot size if you cannot ensure full contact with the sapphire window.
• Test pulses are always advised. Observe laser-tissue interaction before proceeding.
• Apply a thin layer of clear gel (such as ultrasound gel) for increased epidermal
protection and patient comfort.
• When treating skin types IV-VI, use a longer pulse duration.
• Ensure each pulse receives both pre and post cooling.
o Pre-cooling the skin prior to each pulse helps to prevent epidermal damage.
o The length of pre and post cooling time required will vary according to size,
color, and depth of vessel.
Larger, darker vessels require longer pre and post cooling.
o The crystal precools the next pulse when using smaller spot sizes.
• Always observe the epidermis during the treatment, watching for signs of damage (blanching or gray
coloration).
o If damage is seen, stop the treatment and apply a cool compress and evaluate the area for possible
complications and wound care.
• Tissue response
o Start with a test pulse, pre-cooling well.
o Gradually shorten the pulse duration until desired pulse duration is reached, then increase the fluence.
o Experienced practitioners may treat an area with more than one pulse after cooling, but be aware of
stacking the energy/heat and the increased likelihood of tissue injury.
o Consider returning to the area in 10 minutes to re-evaluate tissue response.
• Leg Veins vs. Facial Telangiectasia
o Increased hydrostatic pressure
o Lower extremity vessels are larger and have increased basal lamina compared to facial telangiectasia
o Difficult access due to deeper location of lower extremity vessels
o Altered cytokine patterns upon vessel injury
• Venous Response to Laser Pulse
o 1064 nm used on vessels greater than 1 mm
o Complete and irreversible stenosis after one pass
o Immediate disappearance of vessel followed by sliver like thread
o Constriction from heated collagen “relaxes” with cooling
o Inflammation and intravascular thrombosis occurs
o Even without complete thrombosis, vein wall is damaged
Thrombus begins to organize over next day
• Do not stack pulses or double pulse.
o For smaller vessels, place pulses adjacent to one another or with a slight overlap.
o For larger vessels, leave at least one spot size untreated between pulses.
• “Popping” and extravasation may occur when a vessel is ruptured.
o Cool and compress the area; purpura may develop.
o Lengthen the pulse duration and/or reduce the fluence or leave space on
subsequent pulses.
• Use extreme caution when treating near the eye.
o Only experienced practitioners should treat periorbital vessels.
o Always use patient eye protection.
o Always point the laser beam away from the eye, and never treat near or within the
orbital rim.
• When treating venous lake, treat only the lesion and not the surrounding tissue
o Do not double-pulse.
o Common endpoints for a venous lake are a dusky or deflated look, it should not turn black.
o The venous lake may feel firm a few minutes after treating, the firmness should dissipate within a few
days.
• Endpoints will vary based on type, size, color, volume, pressure, and location of vein.
o Common endpoints are color change, vein disappearance, or constriction.
o If the clinical endpoint is not reached, shorten the pulse duration. If clinical endpoint still not reached,
then increase the fluence.
o The endpoint may not be evident or may be very subtle when treating larger reticular leg veins.
Telangiectasia prior to pulse