Percutaneous Lead Placement in the Epidural Space
Clinician Manual
97035873-01 25 of 75
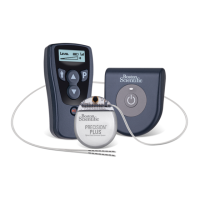
8. While holding the lead stylet handle, place the steering cap over the proximal end of the stylet handle
with moderate force until it is held in place. The lead stylet should be fully inserted into the lead. Slowly
insert the Innion CX Lead into the slotted needle, directing the distal lead tip into the needle lumen.
OPTIONAL. Cover slotted needle with nger to aid in insertion of Innion CX lead into slotted needle
lumen.
OPTIONAL. If needle steering within the slotted needle is not needed, remove slotted needle and insert
lead directly into sheath.
9. OPTIONAL. If exchange of the lead stylet is desired, carefully pull out the existing stylet and insert the
preferred stylet. The stylet must be inserted into the Innion CX Lead tail with one marker band. While
inserting the stylet into the lead, if resistance is encountered, withdraw the stylet approximately 3 cm,
rotate the lead and/or stylet, and gently advance the stylet. If resistance is still encountered, repeat the
above procedure until the stylet can be fully inserted.
The stylet must be inserted into the Innion CX Lead tail with one marker band
WARNING: Do not exchange the lead stylet while the electrode array of the lead is in the bevel of the
insertion needle. If the electrode array is in the bevel area, remove the lead from the insertion needle
before exchanging the stylet. Inserting the lead stylet in the lead while the electrode array is in the bevel
of the insertion needle increases the risk of lead and tissue damage.
WARNING: If the lead stylet is removed and reinserted, do not use excessive force when inserting the
stylet into the lead. The use of instruments, such as forceps, to grasp the stylet during insertion is not
recommended as this could result in applying excessive force and could increase the risk of lead and
tissue damage.
10. Advance the lead to the appropriate vertebral level under uoroscopic guidance. A sufcient length of
lead (at least 10 cm, or approximately three vertebrae) should reside in the epidural space to aid in lead
stabilization.
11. Proceed to the instructions for connecting to the OR Cable assembly in the appropriate DFU for your SCS
System, as listed in your Reference Guide.
 Loading...
Loading...