14
INTRODUCTION SETUP GUIDE
REMOTE
CONTROL PC UTILITIES
DETAIL
SPECIFICATIONS
TROUBLE-
SHOOTING
The "sniffing" position aligns the trachea for the best view of
the glottis and vocal cords when properly using a laryngoscope.
Cricoid pressure may be used by the simulation team member.
The SimNewB™ manikin jaw is realistically hinged and flexible,
for airway and intubation maneuvers.
The SimNewB manikin vocal cords are realistically shaped and
at a depth of 9.5 cm from the upper lip. If the ET tube is inser-
ted too far, it will pass into the right main bronchus, giving only
right side chestrise during positive-pressure ventilation. The
breath sounds on the left side of the chest then disappear.
An ET tube may be secured by means suitable for a neonatal
baby. Tape residues should be cleaned off the skin with soap
and water.
To simulate airway obstructions or very low lung compliance,
the instructor can select the lungs to be partially or fully closed.
Oropharyngeal or nasal pharyngeal airways suitable for neona-
tes may be used.
Lubricate the oropharyngeal or pharyngeal airways before inserti-
on.
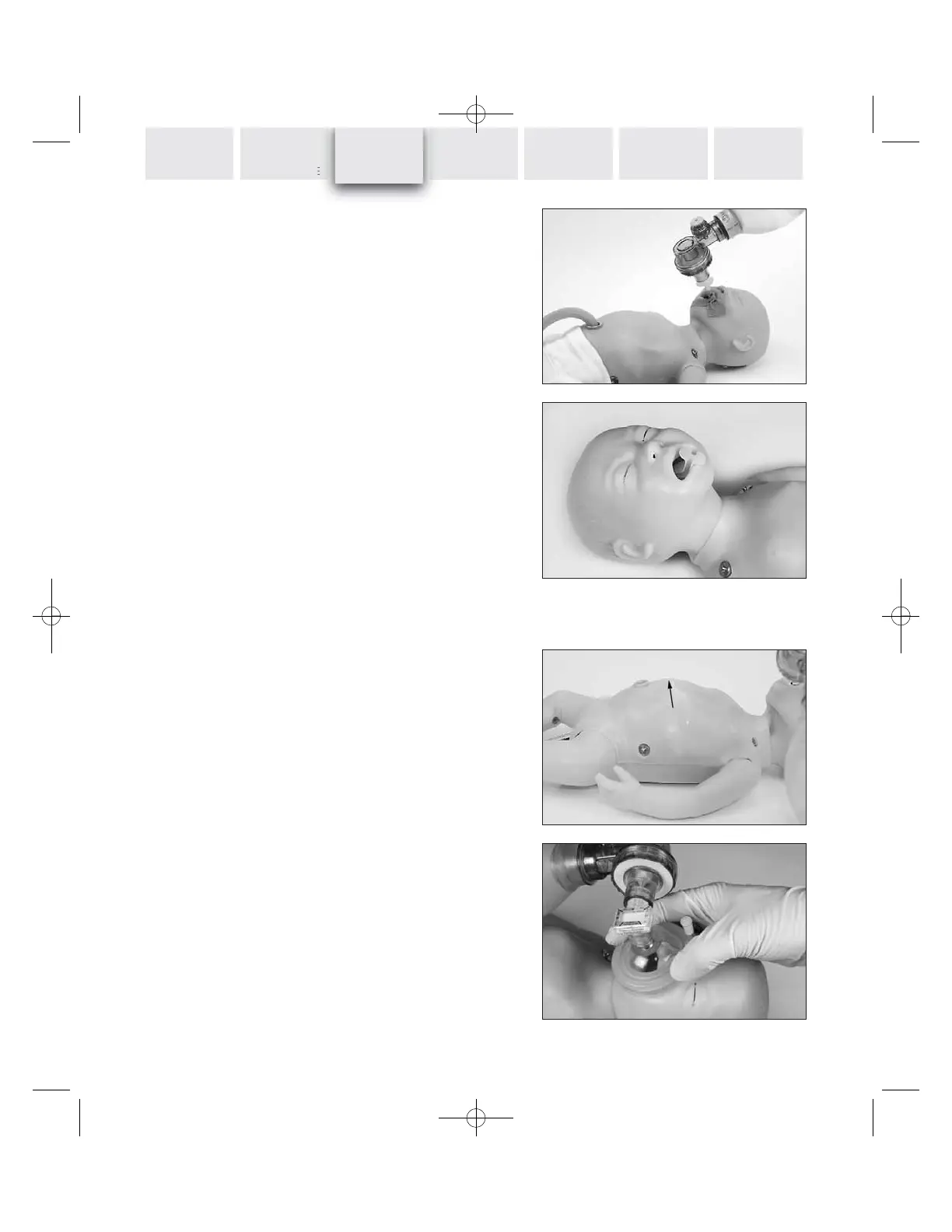
Detection of esophageal intubation
If the esophagus is intubated instead of the trachea, the abdo-
men will then visibly distend for each positive-pressure ventilati-
on.
Stomach ventilation is detectable with the stethoscope.
A capnographic sensor suitable for neonatal use can be used to
detect ETCO
2
output, for example as a means to confirm tra-
cheal intubation contrary to esophageal intubation.
CLINICAL
SIMULATION