A-8
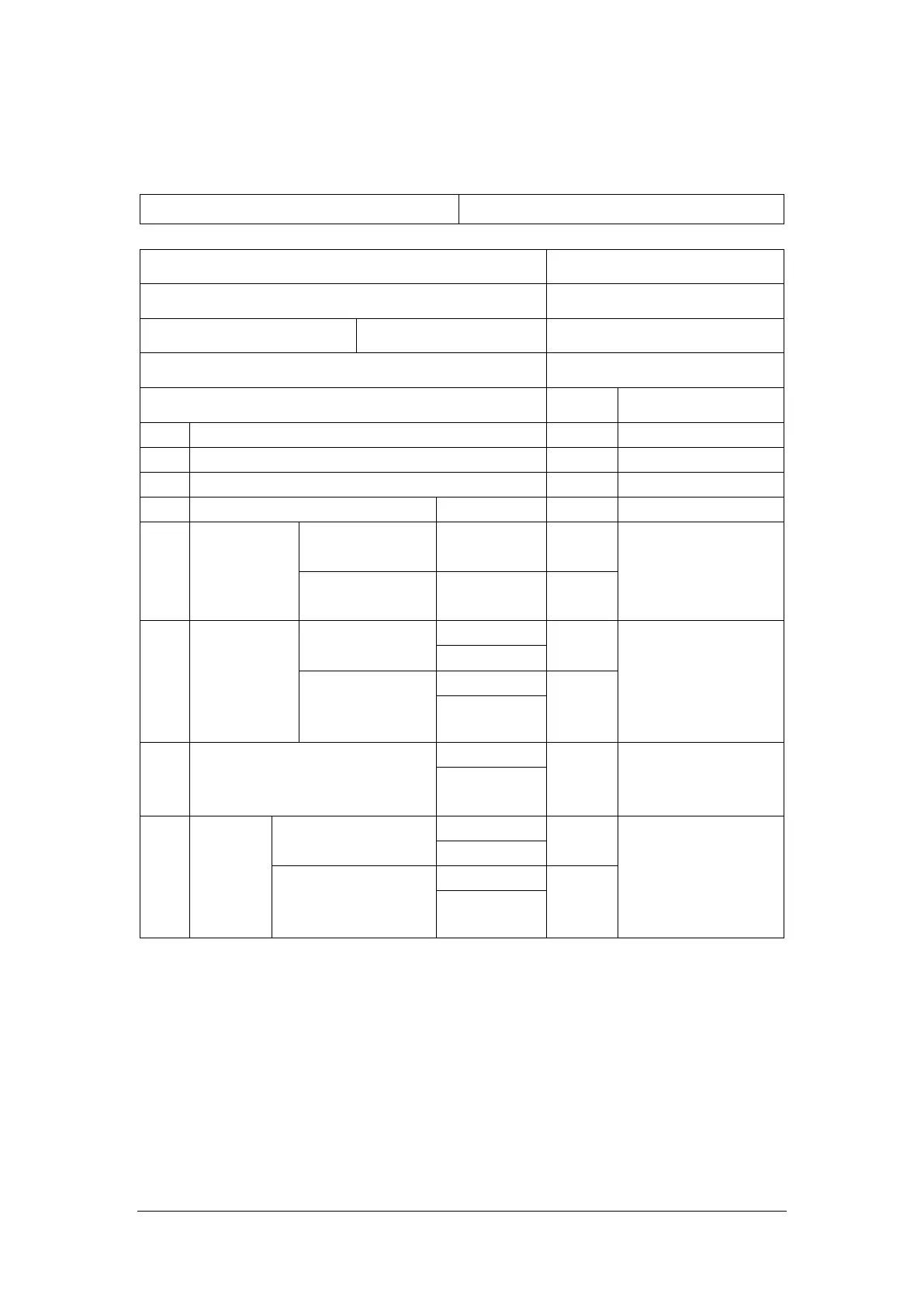
ELECTRICAL SAFETY INSPECTION FORM
Overall assessment:
Scheduled inspection Test item: 1, 2, 3, 4, 5, 6, 7, 8
Location: Technician:
Equipment: Control Number:
Manufacturer: Model: SN:
Measurement equipment /SN: Date of Calibration:
INSPECTION AND TESTING Pass/Fail Limit
1 Power Cord Plug
2 Device Enclosure and Accessories
3 Device Labeling
4 Protective Earth Resistance Ω Max 0.2 Ω
5 Earth Leakage
Normal
condition(NC) ____μA
Max:
NC: 5mA
SFC: 10mA
Single Fault
condition(SFC) ____μA
6
Patient
Leakage
Current
Normal
condition(NC)
□BF____μA Max:
CF applied part:
NC:10μA, SFC: 50μA
BF applied part:
NC:100μA, SFC: 500μA
□CF____μA
Single Fault
condition(SFC)
□BF____μA
□CF____μA
7 Mains on Applied Part Leakage
□BF____μA Max:
CF applied part: 50μA
BF applied part: 5000μA
□CF____μA
8
Patient
Auxiliary
Current
Normal condition(NC)
□BF____μA Max:
CF applied part:
NC:10μA, SFC: 50μA
BF applied part:
NC:100μA, SFC: 500μA
□CF____μA
Single Fault
condition(SFC)
□BF____μA
□CF____μA
Name/ Signature: __________________________ Date:_____________________________