Page 12-10 LTV
®
Series ventilator Operator’s Manual
p/n 10664, Rev. Y
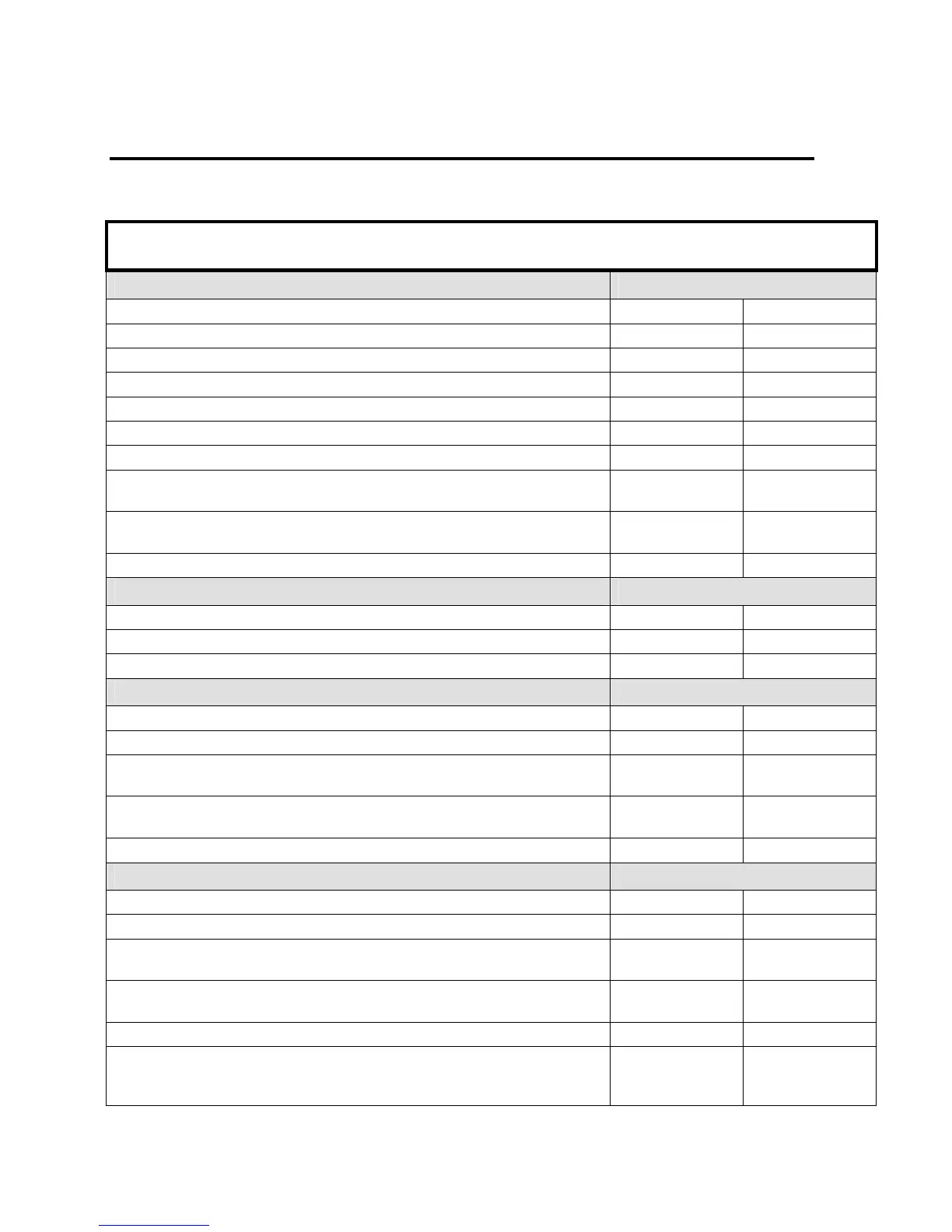
LTV® Ventilator Settings Checklist
The LTV
®
Ventilator Settings Checklist may be used by caregivers as a reminder that all appropriate
controls on the LTV
®
were properly set, adjusted and/or recorded.
Patient Name:
Ordered
By: Date:
Controls: (Fill in (x.x), or Confirm (X)) Monthly Check-up
Volume Mode: - or - Pressure Mode By: Date:
Assist Control: - or - SIMV By: Date:
Breath Rate: bpm By: Date:
Tidal Volume: ml By: Date:
Pressure Control: cmH
2
O By: Date:
Inspiratory Time: Seconds By: Date:
Pressure Support: cmH
2
O By: Date:
High Pressure O
2
%:
(LTV
®
1000)
FIO
2
By: Date:
Low Pressure O
2
%:
(LTV
®
1000/950/900)
Lpm
By: Date:
Sensitivity: Lpm By: Date:
Alarms: (Fill in (x.x), or Confirm (X))
Monthly Check-up
High Pressure Limit: cmH
2
O By: Date:
Low Pressure Limit: cmH
2
O By: Date:
Low Minute Volume: Liters By: Date:
Extended Features-Alarms: (Fill in (x.x), or Confirm (X))
Monthly Check-up
Apnea Interval: Seconds By: Date:
High f HIGH f OFF - or - bpm By: Date:
High PEEP HI PEEP
OFF
- or - cmH
2
O By: Date:
High Pressure Alarm
Delay:
YES - or - NO By: Date:
LPP Alarm: All Breaths - or - VC/PC Only By: Date:
Extended Features-Ventilator: (Fill in (x.x), or Confirm (X))
Monthly Check-up
Rise Time Profile: (1 to 9) By: Date:
Flow Termination: 10-40% of Peak Flow By: Date:
Pressure Support Time
Termination:
Seconds
By: Date:
Pressure Control Flow
Termination:
YES - or - NO By: Date:
Leak Compensation: ON - or - OFF By: Date:
NPPV Mode: (ON means
no audible Low Pressure
or LMV alarms)
ON - or - OFF By: Date: