ECG Monitoring
8-7
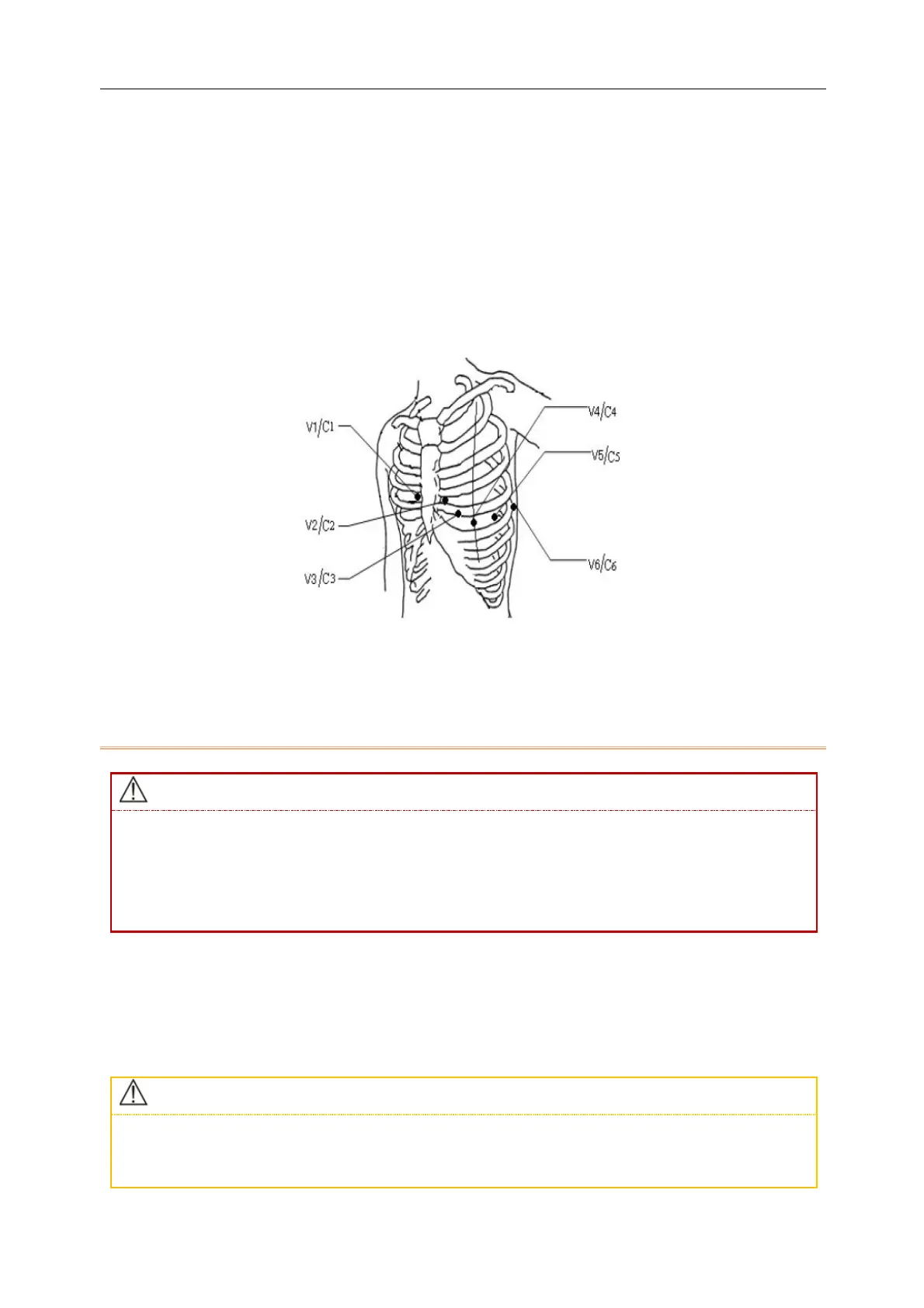
There are generally six electrode positions on the chest, using intercostal gap to pinpoint the positions, V1 ~ V6:
V1: 4
th
intercostal space, at the right sternal border.
V2: 4
th
intercostal space at the left sternal border.
V3: In the middle position between C2 and C4.
V4/C4: 5
th
intercostal space at the left mid-clavicular line.
V5/C5: on the left anterior axillary line, horizontal with the C4 electrode position.
V6/C6: on the left mid-axillary line horizontal with the V4 electrode position.
8.3.3.5 Recommended ECG Lead Connections for a Surgical Patient
When using an ESU, never place electrodes close to the ground plate of the ESU; otherwise there is too
much interference against the ECG signal.
When the monitor is connected to an electrosurgical unit (ESU), in order to protect the patient from
injury caused by leakage current, do not put the sensors and cables of the equipment in contact with
the ESU.
The placement of ECG lead depends on the type of operation to be performed. For example, when a thoracotomy
is to be performed, the electrode can be placed on the side of the chest or on the back. In the OR, artifacts may
affect ECG waveforms due to the use of an ESU. In order to reduce artifacts, the electrodes can be placed at the left
and right shoulders, close to the left and right sides of the abdomen; the chest lead can be placed left to the middle
of the chest. Avoid placing the electrode on the upper arm, or the ECG waveform may become very small.
When monitoring the patient with a pacemaker, [Pacer] must be set to [On]. If it is set to [Off],
pacemaker pulses may be counted as QRS complex, resulting in failure to detect asystole. When
changing patient info or admitting/discharging a patient, check whether [Pacer] is set correctly.